



Social Dilemma: Is paying billions for condoms & contraceptives to "Illegals" worth it?

I don’t like the word “illegals” and I use to think the better word was “undocumented” or in other circumstances the phrase “working uninsured” was more applicable. But I get it, illegals it is.
Some say pay a dollar now or pay a hundred down the road for abortions, baby deliveries, etc., etc.. Before I take you deeper than you could have ever imagined I just wanted to take your temperature now before your brain really gets cooked.
Grab a note pad folks I’m about to take you deep into the jungle.
If you said yes spend a dollar now on birth control to save thousands down the road, you also voted to dispense condoms, lubes, and pills at Jr high and High Schools around the country. Just the “tip” Señorita. I wonder how many “illegals” end up delivering babies through the Medicaid program?
Have you ever heard of Medicaid’s Family Planning Program? Almost every state has one so let’s look at the biggest in the nation, the one in California called California’s Medicaid Family Planning, Access, Care, and Treatment (Family PACT) Program.
Historical data and context from California’s Department of Health Care Services (DHCS) and related reports, adjusted for 2025.:
Key Points on Family PACT Costs:
Program Scope: Family PACT, a California-specific Medicaid State Plan Amendment (SPA) program, provides comprehensive family planning services (contraceptives, STI testing/treatment, counseling, etc.) to low-income individuals (men and women) with incomes at or below 200% of the Federal Poverty Level who are not otherwise eligible for full-scope Medi-Cal (California’s Medicaid program). It serves both citizens and non-citizens, including undocumented individuals, and covers services without cost-sharing.
Funding Structure: Family PACT is jointly funded by federal and state taxpayers. The federal government provides a 90% Federal Medical Assistance Percentage (FMAP) for family planning services, meaning the state covers 10% of service costs. Administrative costs are matched at a 50% federal rate. In 2023, total Medicaid spending in California was approximately $139 billion, with Family PACT as a small but significant component due to its high FMAP.
Historical Cost Data:
In fiscal year (FY) 2018–19, Family PACT served 912,000 clients with a total program expenditure of about $374 million, according to DHCS reports. This included federal (90%) and state (10%) contributions for services, plus administrative costs.
A 2017 report estimated Family PACT’s annual cost at $368 million, serving around 1 million clients. Adjusting for inflation (using CPI medical care rates, approximately 20% from 2017 to 2025), this translates to roughly $442 million in 2025 dollars.
Per-client costs vary by service intensity. In 2018, the average cost per client was about $410 (vaginal/contraceptive visits: $300–$400; STI-related visits: up to $600). With inflation, 2025 per-client costs are likely $500–$700.
Enrollment Trends: Enrollment has declined slightly due to expanded Medi-Cal eligibility under the Affordable Care Act (ACA), which shifted some clients to full-scope Medi-Cal. In 2021, Family PACT served 800,000–900,000 clients, down from a peak of 1.3 million in the early 2000s. Assuming stable enrollment (850,000 clients) and an average cost of $600 per client in 2025, total costs could approximate $510 million annually.
Taxpayer Breakdown:
Federal Share: 90% of service costs (~$459 million, assuming $510 million total) plus 50% of administrative costs (estimated at $10–$20 million total, so $5–$10 million federal).
State Share: 10% of service costs (~$51 million) plus 50% of administrative costs ($5–$10 million).
Total Taxpayer Cost: Approximately $510–$530 million, with federal taxpayers covering ~88–90% ($464–$479 million) and California state taxpayers covering ~10–12% ($56–$61 million).
Contextual Factors:
Cost Savings: Family PACT generates significant savings by preventing unintended pregnancies, which reduces Medi-Cal costs for prenatal care, delivery, and infant care. A 2017 study estimated that every $1 spent on Family PACT saved $5.60 in Medi-Cal costs for pregnancy-related services (e.g., $12,500–$20,000 per birth, as noted in your prior question). In 2018, Family PACT prevented an estimated 200,000 unintended pregnancies, saving Medi-Cal $1.2–$2 billion annually.
Service Utilization: Costs are driven by high-demand services like long-acting reversible contraceptives (LARCs, e.g., IUDs, implants), which are expensive upfront but cost-effective long-term, and STI testing/treatment. Over 70% of clients are women, and 60% are Hispanic, reflecting California’s demographics.
Budget Integration: Family PACT is funded through California’s Medi-Cal budget, with state funds from the General Fund and federal funds via CMS. The 2023–24 California budget allocated $12.7 billion in state funds for Medi-Cal (total $139 billion with federal funds), but Family PACT’s specific allocation is not itemized in public budgets, complicating precise estimates.
Estimate for 2025:
Based on the above:
Total Annual Cost: $510–$530 million, assuming 850,000 clients at $600–$625 per client.
Federal Taxpayer Expense: $464–$479 million (90% of services + 50% of admin).
State Taxpayer Expense: $56–$61 million (10% of services + 50% of admin).
Net Taxpayer Burden: The program’s high federal match reduces California’s fiscal burden, but total costs reflect a small fraction (<0.4%) of Medi-Cal’s $139 billion annual budget. Savings from prevented pregnancies likely offset much of the expense, making Family PACT cost-neutral or cost-saving for taxpayers overall.
Limitations and Sources:
Data Gaps: No 2024–25 DHCS report provides exact Family PACT costs. Estimates rely on 2017–19 data, inflation adjustments, and enrollment trends. CMS or DHCS could provide unpublished data.
Sources Used:
DHCS Family PACT reports (2018–19 data).
KFF Medicaid financing reports (2023 spending, FMAP).
California Medi-Cal budget summaries (2023–24).
Next Steps: For a precise figure, contact DHCS or CMS, or check California’s 2025–26 budget (released June 2025).
How many states have similar Family Planning Programs?
To determine how many states have a Medicaid family planning program similar to California’s Family Planning, Access, Care, and Treatment (Family PACT) Program, we need to define “similar” and examine Medicaid family planning expansions across states. Family PACT is a State Plan Amendment (SPA) program that provides comprehensive family planning services (contraceptives, STI testing/treatment, counseling, etc.) at no cost to low-income individuals (up to 200% of the Federal Poverty Level, FPL) who lack other coverage for these services, including men and women of all reproductive ages, with a focus on accessibility, confidentiality, and on-site enrollment. It’s administered by California’s Department of Health Care Services (DHCS) and serves a large population (historically 800,000–1.3 million annually).
Definition of “Similar” Programs
A program is considered similar to Family PACT if it:
Extends Medicaid eligibility for family planning services to individuals who wouldn’t otherwise qualify for full-scope Medicaid (e.g., based on income up to 200% FPL or higher).
Covers comprehensive family planning services (e.g., contraceptives, STI testing/treatment, counseling) with minimal or no cost-sharing.
Operates as a standalone or limited-scope program, separate from full-scope Medicaid, often via a State Plan Amendment (SPA) or Section 1115 Waiver.
Targets low-income individuals, including those without other insurance, and may emphasize confidentiality or accessibility (e.g., on-site enrollment, broad provider networks).
Medicaid Family Planning Expansions Nationwide
Medicaid family planning programs are common, as all states must cover some family planning benefits under federal rules. However, many states have expanded eligibility for these services to reach populations not eligible for full-scope Medicaid, often through SPAs or Section 1115 Waivers. These expansions began in the 1990s and were streamlined by the Affordable Care Act (ACA) in 2010, which allowed states to establish SPAs without needing to renew waivers.
Based on available data:
Kaiser Family Foundation (KFF) Reports: As of January 2016, 14 states had adopted family planning SPAs to extend Medicaid eligibility for family planning services. By 2022, KFF noted that “more than half of states” (at least 26 states) had established programs expanding Medicaid eligibility for family planning services to individuals who wouldn’t otherwise qualify. These programs typically use income-based eligibility (e.g., 185–250% FPL) and cover prescription contraceptives, STI testing/treatment, and counseling.
Guttmacher Institute (2019): Identified 24 states with Medicaid family planning eligibility expansions, either through SPAs or waivers, targeting low-income individuals not eligible for full-scope Medicaid.
2017 KFF Case Studies: Highlighted six states (Alabama, California, Connecticut, Illinois, Missouri, Virginia) with family planning programs, noting variations in structure. For example:
Alabama’s Plan First: A Section 1115 Waiver program for women aged 19–55 with incomes up to 141% FPL, covering contraceptives and STI services but not men.
Connecticut: Uses presumptive eligibility for temporary coverage, similar to Family PACT’s on-site enrollment.
North Carolina’s Be Smart: Covers individuals of all reproductive ages and genders with incomes up to 195% FPL, resembling Family PACT’s broad eligibility.
Recent Trends: As of 2024, at least 28 states have some form of Medicaid family planning expansion, per KFF’s state fact sheets and Medicaid policy updates. This includes states maintaining programs post-ACA, as they serve unique roles (e.g., confidentiality, access for those ineligible for full-scope Medicaid).
States with Programs Most Similar to Family PACT
While 28 states have family planning expansions, not all match Family PACT’s scope, scale, or features. Key similarities include income eligibility (around 200% FPL), comprehensive services, and accessibility. Based on detailed comparisons:
States with SPAs (14 as of 2016, likely 16–18 by 2025): SPAs are closest to Family PACT, as they permanently extend eligibility without waiver renewals. Examples include:
California (Family PACT): Income up to 200% FPL, no age/gender limits, 2,200 providers, on-site enrollment, confidential.
New York: Family Planning Benefit Program (FPBP) covers men and women up to 200% FPL, with comprehensive services and confidentiality.
Oregon: Reproductive Health Equity Program, covering family planning for low-income residents, including non-citizens, up to 250% FPL.
Washington: Take Charge, a waiver program (converted to SPA in some reports), covers men and women up to 260% FPL.
States with Waivers (10–12 as of 2024): Section 1115 Waivers are less permanent but can mimic Family PACT’s scope. Examples:
Alabama (Plan First): Women only, up to 141% FPL, less comprehensive than Family PACT.
North Carolina (Be Smart): All genders, up to 195% FPL, comprehensive services, similar to Family PACT but smaller scale.
South Carolina: Family Planning Program, covers women up to 194% FPL, with some male services.
Other Notable Programs:
Connecticut: Presumptive eligibility and broad service coverage, akin to Family PACT’s accessibility.
Illinois: Limited-scope program for family planning, less extensive provider network than Family PACT.
Wisconsin: Family Planning Only Services, covering men and women up to 300% FPL, with a focus on contraceptives and STI care.
Estimate of Similar Programs
Total States with Expansions: Approximately 28 states have Medicaid family planning programs that extend eligibility beyond full-scope Medicaid, per KFF and Guttmacher data.
States with “Similar” Programs: Around 15–20 states have programs closely resembling Family PACT in terms of income eligibility (185–250% FPL), comprehensive services (contraceptives, STI care, counseling), and accessibility (e.g., on-site enrollment, confidentiality). This includes:
SPA States (14–18): California, New York, Oregon, Washington, Maryland, New Mexico, Rhode Island, and others, which prioritize broad eligibility and comprehensive care.
Waiver States (3–5): North Carolina, Connecticut, and possibly South Carolina, with programs mirroring Family PACT’s scope and accessibility.
Exclusions: States like Alabama, Missouri, or Virginia have narrower programs (e.g., women-only, lower income thresholds, or limited services), making them less similar to Family PACT.
Why the Range?
Data Gaps: Exact numbers fluctuate due to evolving state policies, ACA impacts, and inconsistent reporting. Some states have transitioned waivers to SPAs, and others have scaled back programs as full-scope Medicaid expanded.
Variability: Programs differ in scale (Family PACT’s 800,000–1.3 million clients is unmatched), provider networks, and inclusion of men or non-citizens. Few replicate Family PACT’s on-site enrollment or confidentiality focus.
Recent Updates: Post-2019 data is limited, but KFF’s 2024 fact sheets suggest 28 states maintain expansions, with 15–20 aligning closely with Family PACT’s model based on eligibility and services.
Final Answer
Approximately 15–20 states have Medicaid family planning programs similar to California’s Family PACT, characterized by income-based eligibility (around 200% FPL), comprehensive services, and accessibility features like confidentiality or on-site enrollment. These include states with SPAs (e.g., New York, Oregon, Washington) and select waiver programs (e.g., North Carolina, Connecticut). For a precise list, contact CMS or check state Medicaid websites, as programs evolve. Would you like me to investigate a specific state’s program for comparison?
Do the other four largest states in the nation have a Medicaid Family Planning Services?
Yes, Texas, Florida, Pennsylvania, and New York each have Medicaid family planning programs that expand eligibility for family planning services to individuals who may not qualify for full-scope Medicaid, similar to California’s Family PACT program. Below is a detailed overview of each state’s program, focusing on their similarity to Family PACT (income-based eligibility around 200% of the Federal Poverty Level, comprehensive services, and accessibility features like confidentiality or broad provider networks).
1. Texas: Family Planning Program (FPP) and Healthy Texas Women (HTW)
Program Description: Texas operates the Family Planning Program (FPP) and Healthy Texas Women (HTW), both funded through Medicaid and state funds, to provide family planning and reproductive health services to low-income women and men. The FPP focuses on clinic-based services, while HTW integrates family planning with broader women’s health services. These programs serve Texas residents ineligible for full-scope Medicaid, with a focus on preventing unintended pregnancies and improving health outcomes.
Eligibility:
FPP: Texas residents aged 64 or younger, with household incomes at or below 250% of the Federal Poverty Level (FPL), who are ineligible for Medicaid or HTW. Services may be provided to individuals with third-party insurance if confidentiality is a concern or if their deductible is 5% or more of monthly income.
HTW: Women aged 15–44 (or 15–17 with parental consent) with incomes up to 200% FPL, including automatic enrollment for women losing pregnancy-related Medicaid after 60 days postpartum.
Services:
Contraceptives (e.g., birth control pills, IUDs, implants, except emergency contraception in FPP), STI testing/treatment, preconception health screenings (e.g., obesity, hypertension, diabetes), cervical/breast cancer screenings, and reproductive health counseling.
FPP excludes emergency contraception but covers long-acting reversible contraception (LARC). HTW covers emergency contraception (e.g., Plan B).
Postpartum depression screening and treatment are included, with specific guidelines in the Texas Clinician’s Postpartum Depression Toolkit.
Accessibility:
Services are provided through a network of clinics (e.g., family planning clinics, health departments, FQHCs) across Texas, with over 2,000 providers.
Confidentiality is emphasized, especially for minors or those with privacy concerns. Income verification may be waived if it jeopardizes confidentiality.
Providers must certify they do not perform or promote elective abortions, per Texas Administrative Code.
Similarity to Family PACT: Texas’ FPP and HTW are highly similar to Family PACT due to their income eligibility (200–250% FPL), comprehensive services (contraceptives, STI care, screenings), and focus on accessibility via a large provider network. However, FPP’s exclusion of emergency contraception and abortion-related restrictions differ from Family PACT’s broader scope. HTW’s inclusion of emergency contraception aligns more closely with Family PACT.
Funding and Scale: Funded by Medicaid (90% federal match for family planning services) and state funds. FPP served 95,000 clients in 2018, while HTW served over 200,000 in 2020, per Texas Health and Human Services (HHS) reports.
2. Florida: Medicaid Family Planning Waiver Program
Program Description: Florida’s Medicaid Family Planning Waiver Program, also called “Family Planning Medicaid for Today’s Woman,” is a Section 1115 Waiver program that provides family planning services to eligible women for up to 24 months. It targets women losing Medicaid eligibility (e.g., after pregnancy) or those ineligible for full-scope Medicaid.
Eligibility:
Women aged 14–55 with family incomes at or below 185% FPL who are not otherwise eligible for Medicaid, CHIP, or health insurance covering family planning services.
Women losing pregnancy-related Medicaid (SOBRA) are automatically enrolled for the first 12 months; others must apply at county health departments. All must reapply after 12 months.
Services:
Family planning exams, contraceptives (e.g., pills, IUDs, implants), STI evaluation/treatment (limited to 6 weeks post-exam), related pharmaceuticals, and lab testing.
Does not cover transportation or abortion services.
Accessibility:
Services are provided through county health departments, clinics, and Medicaid-enrolled providers. Applications require proof of identity and income, except for auto-enrolled postpartum women.
Confidentiality is ensured, especially for minors (aged 14+), per Florida’s minor consent laws for reproductive health.
Similarity to Family PACT: Florida’s program is moderately similar to Family PACT due to its income eligibility (185% FPL), comprehensive services, and confidentiality focus. However, it is less similar because it excludes men, limits STI treatment duration, and requires active reapplication (unlike Family PACT’s on-site enrollment). The 24-month coverage cap is also more restrictive than Family PACT’s ongoing eligibility.
Funding and Scale: Funded by Medicaid with a 90% federal match. In 2018, the program served approximately 50,000 women, per Florida Agency for Health Care Administration (AHCA) data.
3. Pennsylvania: Family Planning Services Program
Program Description: Pennsylvania’s Family Planning Services Program provides family planning and related services to men and women who are not otherwise eligible for full-scope Medical Assistance (Pennsylvania’s Medicaid program). It operates as a limited-scope Medicaid program, integrated into the state’s Medicaid framework.
Eligibility:
Men and women with incomes at or below 215% FPL who are not eligible for other Medicaid categories.
No age restrictions, though services target those of reproductive age.
Services:
Contraceptives (e.g., pills, IUDs, condoms), STI testing/treatment, HPV vaccine, family planning drugs (e.g., antibiotics for STIs), and screenings for genito-urinary infections.
Covers over-the-counter contraceptives (e.g., condoms) without a prescription, unlike many states.
Utilization controls include quantity limits on LARCs based on FDA guidelines.
Accessibility:
No special provider enrollment is required; any Medicaid-enrolled provider offering family planning services can participate.
Services are free and confidential, with billing through standard Medicaid processes.
Similarity to Family PACT: Pennsylvania’s program is very similar to Family PACT due to its income eligibility (215% FPL), inclusion of men and women, comprehensive services (including OTC contraceptives without prescriptions), and accessibility through a broad Medicaid provider network. The lack of presumptive eligibility or on-site enrollment makes it slightly less flexible than Family PACT.
Funding and Scale: Funded by Medicaid with a 90% federal match. Exact client numbers are unavailable, but Pennsylvania’s Medicaid program served 3.2 million people in 2023, with family planning as a key benefit.
4. New York: Family Planning Benefit Program (FPBP)
Program Description: New York’s Family Planning Benefit Program (FPBP) is a Medicaid State Plan Amendment (SPA) program providing free, confidential family planning services to teens, women, and men who meet income and residency requirements and are not enrolled in full-scope Medicaid. It emphasizes accessibility and confidentiality, especially for those seeking services without other insurance involvement.
Eligibility:
Individuals of childbearing age with incomes up to 223% FPL, who are U.S. citizens, nationals, Native Americans, or lawfully present.
Eligible even if covered by other insurance (e.g., Child Health Plus) if seeking confidential services, but not if already on Medicaid (since Medicaid includes family planning).
Services:
All FDA-approved contraceptives (e.g., pills, IUDs, implants, condoms), STI testing/treatment, HIV testing/counseling, Pap smears, pelvic exams, breast/cervical cancer screenings, and reproductive health counseling.
Covers OTC contraceptives (e.g., condoms, Plan B) without a prescription, enhancing access.
Accessibility:
Provided through 2,700+ providers, including hospitals, family planning clinics, health departments, FQHCs, OB/GYNs, midwives, and pharmacies.
Presumptive eligibility screenings and on-site enrollment at Family Planning Program Sites ensure rapid access, similar to Family PACT.
Confidential services are guaranteed, with no need for prior approval from other health plans.
Similarity to Family PACT: New York’s FPBP is highly similar to Family PACT due to its income eligibility (223% FPL), inclusion of men and women, comprehensive services (including OTC contraceptives without prescriptions), large provider network, and accessibility features like presumptive eligibility and on-site enrollment. It matches Family PACT’s focus on confidentiality and rapid access, making it one of the closest analogs.
Funding and Scale: Funded by Medicaid with a 90% federal match. In 2018, FPBP served approximately 100,000 clients, per New York State Department of Health data.
Summary and Comparison to Family PACT
All Four States Have Similar Programs:
Texas (FPP/HTW): Very similar (200–250% FPL, comprehensive services, large provider network), but FPP excludes emergency contraception, and abortion restrictions limit provider participation.
Florida (Family Planning Waiver): Moderately similar (185% FPL, comprehensive services, confidential), but excludes men, has a 24-month cap, and requires reapplication, making it less flexible.
Pennsylvania (Family Planning Services): Very similar (215% FPL, includes men/women, OTC contraceptives without prescriptions), but lacks presumptive eligibility.
New York (FPBP): Extremely similar (223% FPL, includes men/women, OTC contraceptives without prescriptions, presumptive eligibility, on-site enrollment), closely mirroring Family PACT’s structure and accessibility.
Key Similarities to Family PACT:
All programs extend eligibility beyond full-scope Medicaid, targeting low-income individuals (185–250% FPL).
They cover comprehensive services (contraceptives, STI care, screenings) with no cost-sharing, funded by a 90% federal match.
Confidentiality is prioritized, especially for minors or those with privacy concerns.
Key Differences:
Florida’s program is women-only and time-limited (24 months), unlike Family PACT’s broader eligibility and ongoing coverage.
Texas’ FPP excludes emergency contraception, and its abortion-related provider restrictions are stricter than Family PACT’s.
Pennsylvania and New York align more closely with Family PACT, but Pennsylvania lacks on-site enrollment, and New York’s provider network (2,700+) is closer to Family PACT’s scale (2,200 providers).
Count Toward Total: All four states contribute to the 15–20 states with programs similar to Family PACT, as their income thresholds, service scope, and accessibility align with Family PACT’s model, despite variations.
Additional Notes
Data Sources: Information is drawn from state Medicaid websites, Kaiser Family Foundation (KFF) reports, and Guttmacher Institute data, supplemented by web results (e.g., for New York, for Florida, for Pennsylvania, for Texas). No exact 2025 data exists, but 2019–2024 sources are reliable for program structure.
Verification: For precise eligibility or provider details, contact state Medicaid agencies (e.g., Texas HHS at 1-800-925-9126, Florida AHCA at 1-877-254-1055, Pennsylvania DHS at 1-800-692-7462, New York DOH at 1-800-541-2831).
National Family Planning Services Calculations by The Eagle:
In all the minutiae above for California with a population of 39.6M and 850K family planning participant at a cost of about $650/yr the annual cost a little over a half billion a year. Let extrapolate.:
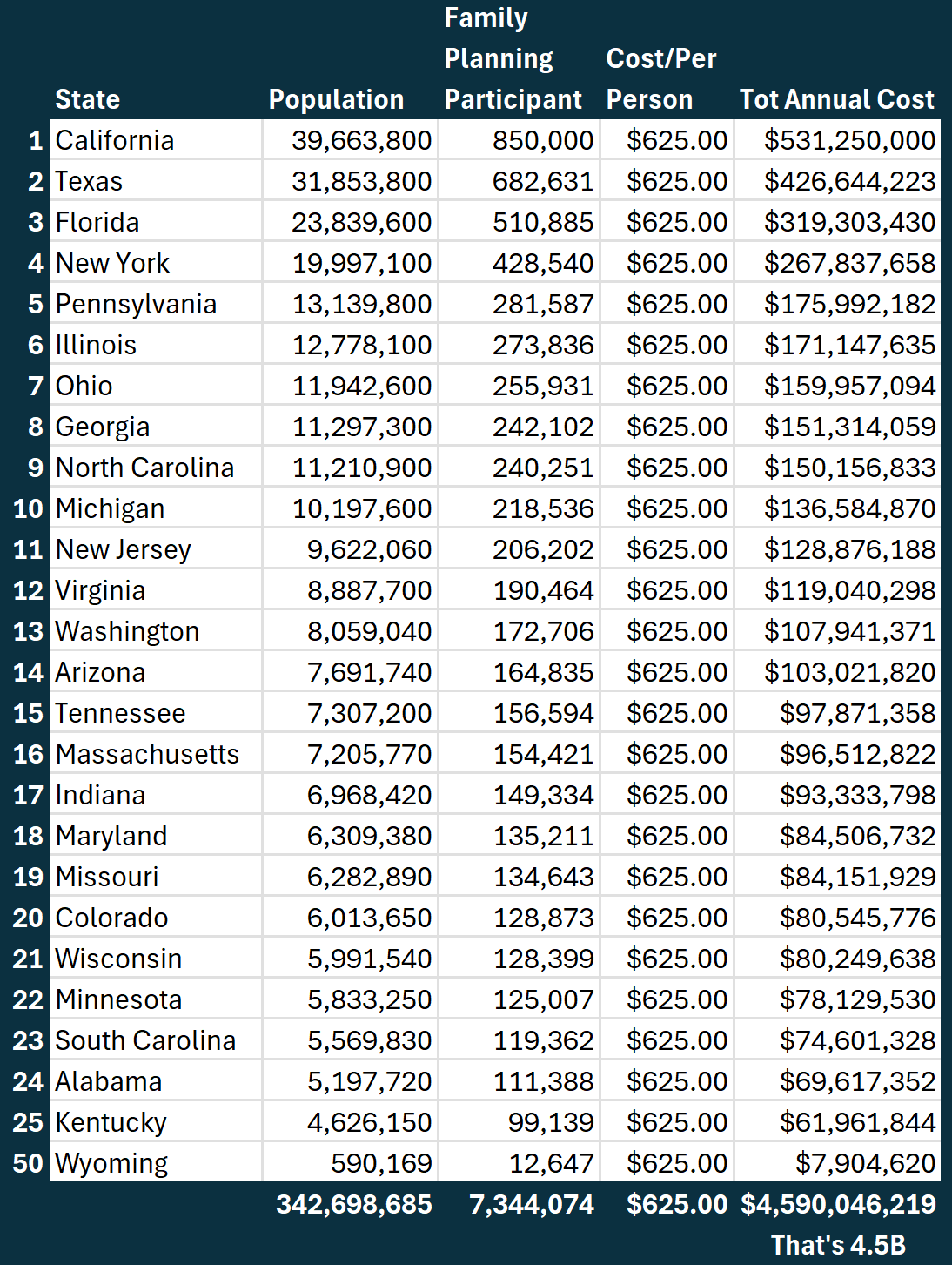
4.5B annual cost might be a tiny sum for all these condoms and birth control pills but who is really getting it? Here is who qualifies
Income - People making under twice the poverty level. That means if the poverty level is considered ~$12K/yr people making under $24K/yr would qualify.
Age - People of child bearing age. That usually all men a girls/ladies 12-55yr olds
Residence - If you slept in the state last night you are considered a resident in this program
Social Security Number - Used to be optional, now says it’s a self reported system, meaning you are on your honor to submit your applicable SS#, but nobody is double checking anything.
Can you see how this program makes it into every progressive high school and junior high in the nation?
Can you see how if Andrew Tate and Fillmore Slim don’t have all their hoes on this program, they just ain’t pimp’n?
This family planning program actually might be George Soros worst nightmare!
Did you know this programs covers contraception up to vasectomy and tubal ligation? It does…
Here is a 61 page benefits grid to show you everything covered:
Here is the California’s Family Planning website:
https://familypact.org/
Like everything else it’s good on paper but it’s getting milked by the wrong people. This is the kind of stuff Dr. Oz, Bobby, Makary, Baty Batts, and Kirsch knows jack shit about. But I’m here to help. Next article coming up will be on the Medicaid’s Presumptive Eligibility Program where the real shady milking goes on. I will also try and show you how all this progressive thinking on handing out condoms in junior high to handing out needles to drug addicts is slowly killing America. God Bless

Mistakes weren’t made, this was/is an attack on humanity. God Bless
Please support The Eagle!
https://www.vaersaware.com/donate
Need help finding your VAERS report?
https://www.vaersaware.com/findmyreportrequest
Please sign Federal Investigation Petition:
https://www.vaersaware.com/fedinvestigation
The best (only) VAERS dashboard:
https://www.vaersaware.com/entire-vaers-1990-current
Admittedly, I could not read the entire article. However, one question is outstanding and should be answered: if illegal/undocumented people were not present in the country, how much money would be saved for giving medical care to US citizens?
It is long past due - suspend habeus corpus now and ship them out!!!
Investigate, indict and jail every SOB who played a role in this illegal invasion!