



Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine in the United States (Part 2)
The deeper dive...

The previous article: HERE
Before I start I want to say I got a positive response from Dr. Brian Hooker…

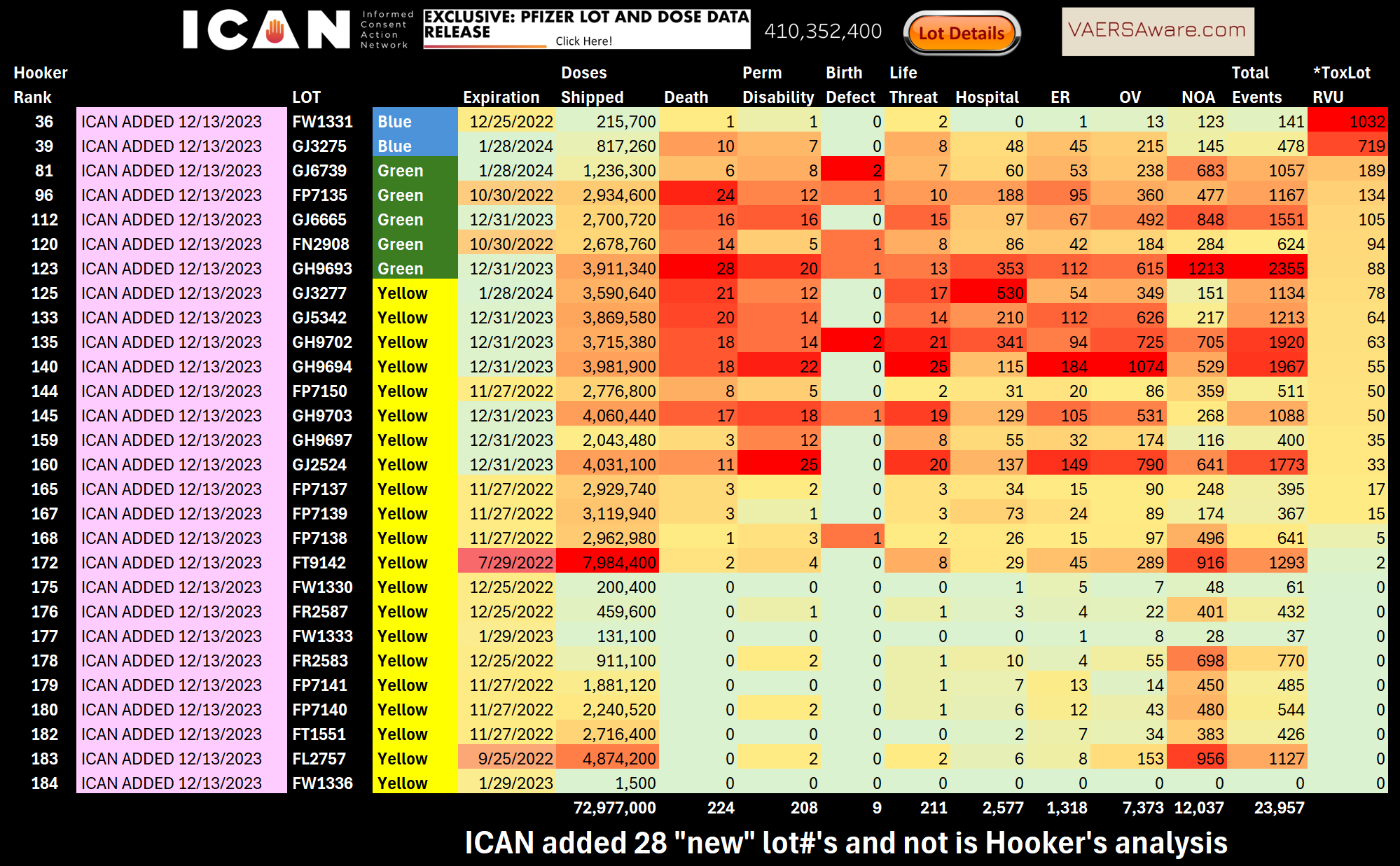
I’ve popped the hood and started looking at the serial numbers on this motor, so let me explain Exhibit A which is the vaersaware.com Pfizer American blue, green, yellow lots as I see it:



The first order of business is the discrepancy between the 410M doses shipped which matched Dr. Hooker’s study versus these 484M doses shipped I’m calculating now. This is important because we want to make sure we are counting the apples and oranges as makes a considerable difference if a lot number with 50 deaths had 1 million doses shipped or 2 million doses shipped?
The reason for this is because ICAN actually had 3 updates total with the last update on December 13, 2023. However the 2023 update is NOT what Dr. Hooker’s study was working from.

The small huge problem with the Dec 2023 update is that it did NOT contain the robust details about the providers these batches were being sent to, like the version Dr. Hooker worked from. I have to believe the CHD team knew this but decided to roll with the previous version from Sept 2022? Nothing wrong with that, but there are some caveats.
There is a clue in Hooker’s Table 1, but I am interested in this mention of 194 discernable lots through Dec 2022? I agree with 156 lots for 410M doses

Was this December 2022 by vax date, or published date, or VAERS received date? The Dec 2023 ICAN update had 185 lot numbers, or 186 if you count lot# NA with 28,170 doses shipped.
So here is when it starts to get a wee bit complicated when reconciling or doing a compare/contrast between the updates. The CDC actually adjusted doses shipped both increasing and decreasing total shipments. The problem is it’s only high level grand totals, so it’s impossible to make the adjustments down to the 46,327 providers, hospitals, pharmacies, and institutions Dr. Hooker describes. I am able to show you these brass tacks.:


We a starting to get deep in the weeds. I am preparing a custom dashboard build out to back-up all my work and assertions. However, I do want to point out something the CHD scientists did super well, or at least it’s technique they chose to use that I call coding event levels to ultimate specificity. Dr. Hooker calls it “worst case outcomes”. This means each case or report aka ID# gets only the highest level event outcome recorded. Here is Hooker’s exact blurb:

Coding event level to ultimate specificity per report is exactly how I built my dashboards since day 1. Thanks Dr. Hooker for having the wisdom to see the value of this technique. Everything is double counted in openvaers, howbadismybatch, and everywhere else. Sometimes it’s good to know which people died at home and which people migrated through an office visit to ER to Inpatient to death, however for the sake to what we are doing here and most studies, coding event levels to ultimate specificity is superior.
I’ve heard the question from the cheap seats many times,… Why don’t all deaths also have Life Threatening and and/or permanent disability checked off as well? Bottom line is it’s all left to the discretion of the submitter and it’s vary arbitrary.
There is something else that is very arbitrary and it’s a snake in the grass particularly with these hot lot/placebo studies. Administration Error only reports!
I want to use Lot FK5127 as an example:

I ranked this lot as #173 on the list, Dr. Hooker points is out as being one of the largest shipped doses 10,556,600. This lot has only 3 deaths but it does have some of the most administrations errors!
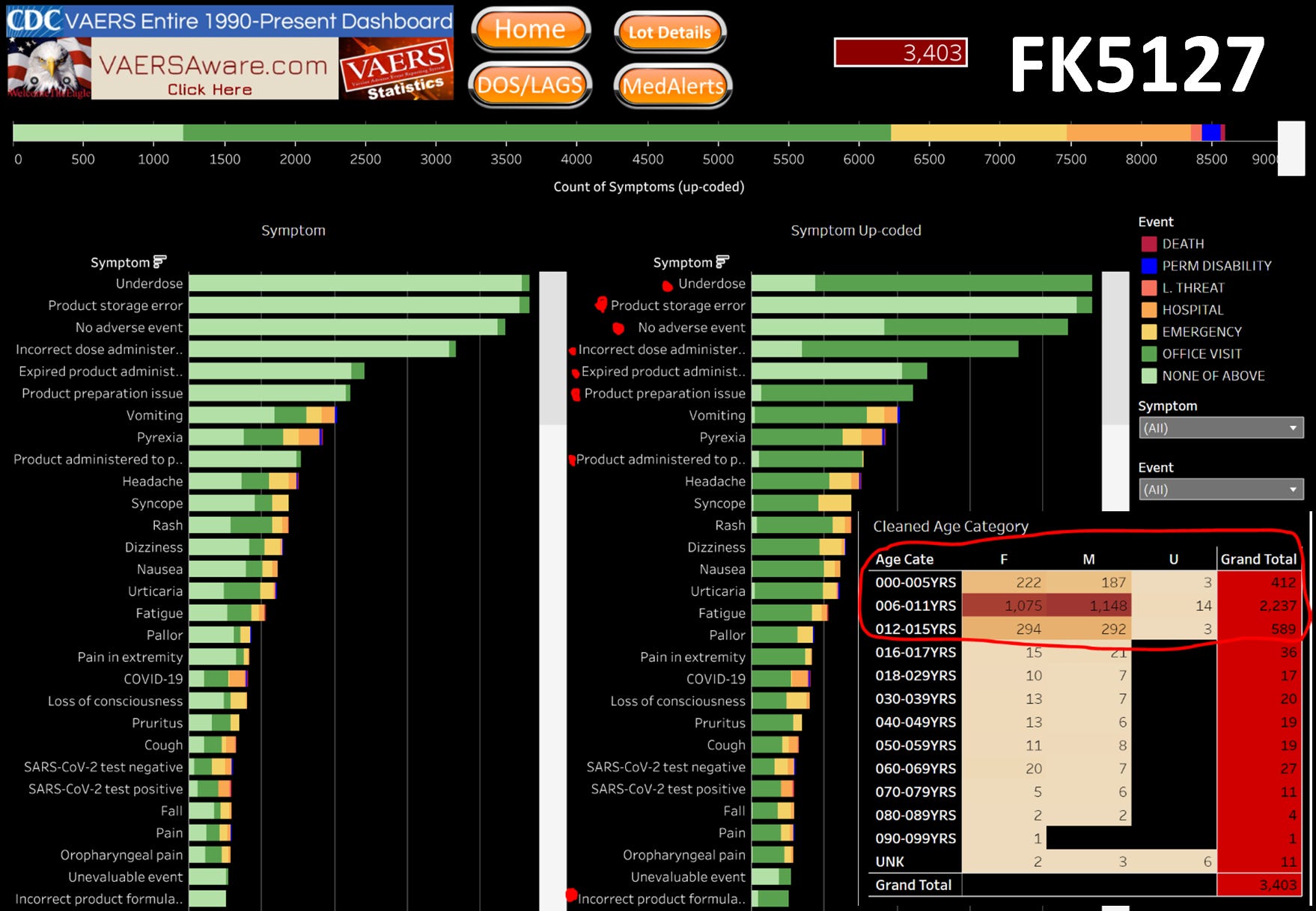
I confirm 2,043 of 3,403 reports for administration error only reports. This seems harmless and almost looks good on paper as good pharmacovigilance process of obligating vaccinators to create reports for every administration error. However, this is now working in the pharma cabal’s favor since only initial reports are published. What happens when the expired dose causes a adverse event after the report has already been filed? What happens when a child of inappropriate age get jabbed and a report is immediately filed for the administration error only?
Do you see now how administration error only reports can skew the some analysis and in the real world hide future injury. Hypothetically VAERS 2.0 needs to have a solution for this like having a extra even level for administration only error reports, with ability to “append” initial report shout a future adverse event arise.
It’s kind of a big problem, I see just shy 120,000 reports with only a administration error only as the report. About 12,000 are coming from foreign countries. About ~52,000 are domestic Pfizer admin error only reports!!
I want to reiterate what a good paper I think this is. However what I’ll keep harping on until I’m blue in the face is the THROTTLING!
I think as long as we keep playing around with these batch dependent studies without putting a bright light on the purposeful delay of publishing reports, we won’t reach the Wizard of Oz pulling off this scam.
Let me rest my case for now by reminding how very old these lots are now in nearly Oct 2024, yet just you watch come this Friday we will still get brand “new” reports published this week against some of these ancient lots!
Here is what we’ve been getting still in 2024…
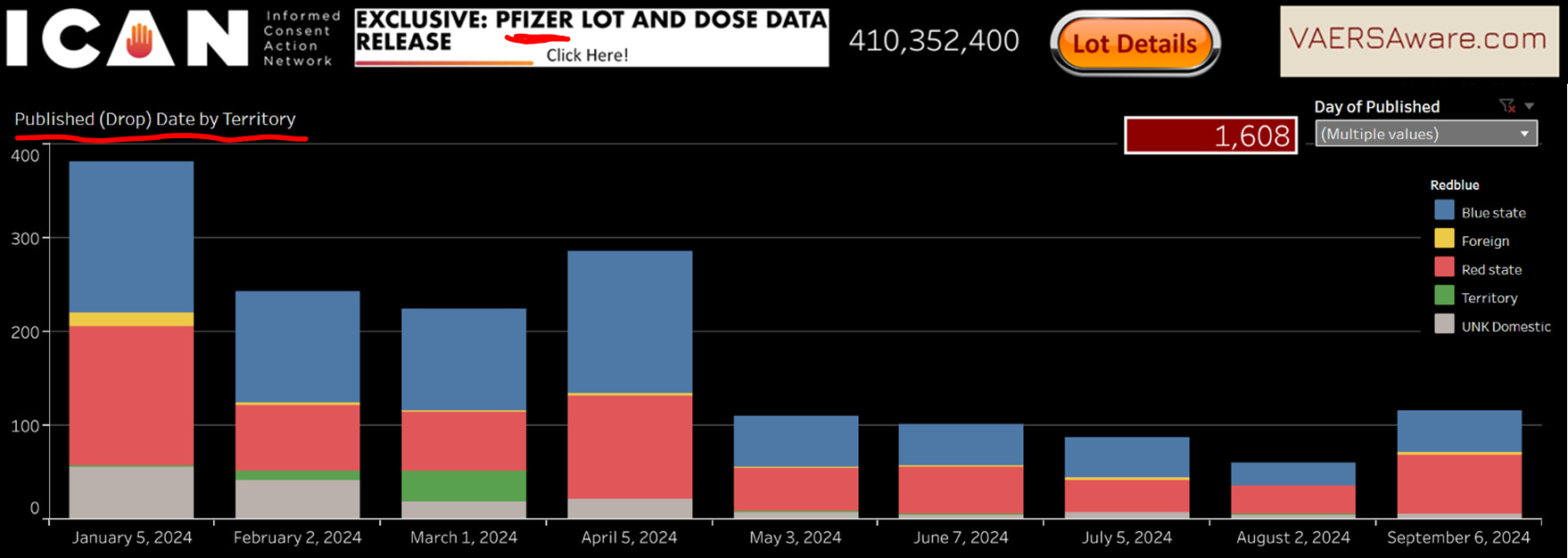
There is about 171 deaths in these ICAN domestic Pfizer 1,608 reports. This is just the older Pfizer ICAN lots, outside of this there plenty more domestic Pfizer lots outside the scope of this study!
ICAN and Aaron Siri have done a lot, but it would be awesome if they could shake the VAERS tree one more time and get a fresh update, with all the details of the initial haul.
If we could get a V-Safe update I’d be happier too.
FYI: Lot number was P000133 was mentioned in this Hooker Study, I think it might be a typo and might be P0001332.
Thank you.
You are the best, Albert. Thanks for giving some kudos to Dr. Hooker, too.