



Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine in the United States
Dr. Brian Hooker & Jablonowski come in strong with a good Pfizer "Hot Lot" Analysis paper, and my analysis of it...


First of all this study is much more transparent than the Denmark study, so thank you Dr. Hooker Dr. Jablonowski for including data sources and supplemental. I know Hooker definitely won’t be saying “harmless, placebo, or saline” batches for the American version of the yellow batches based on this proof here:

In Dr. Hooker’s American version of Pfizer’s arbitrary yellow batches, you will notice the “yellow” cluster includes 29 batches which included 212 deaths, 4,697 Serious Adverse Events. There is three clusters or groups that seem to have emerged just like the Denmark study but it’s arbitrary in the sense that it could easily be four groups or five groups, or 8 groups just like their is 8 adverse event levels.
Speaking of Adverse Event “severity” (SAE) we can for the sake of interpretation consider severe or serious to mean the same thing. One huge disclaimer needs to be defined here, Dr. Hooker’s definition of serious adverse event (SAE) in this study means AE levels Emergency, Hospitalizations (and extended stays), Life Threatening, Birth Defect, Permanent Disability, and Death. This just leaves off Office Visits and None of Above (NOA). NOA’s is the event level where 65% of all Covid-19 reports reside, that’s a million reports. This is huge because under-coding is one of the biggest Las Vegas tricks VAERS pulls off. There’s even about ~40 uncounted deaths in NOA presently.

However, by CDC’s own definition a “serious” event is anything “hospitalization” or higher. I agree with Hooker and everybody else who includes ER visits as serious in these studies, it just has to be stated as Hooker has done. Miscarriages and fetal demises are the best example of inadvertent under-coding in VAERS as most fetal demise does not rise to the level of a in-patient hospitalization and therefore are not considered “serious”. I think it’s ethically appropriate to place all miscarriages and demises at the Birth Defect/Congenital Anomaly where applicable, this way they could be officially considered serious.

On the flip side and in practical application, regular people on the street like the working uninsured or Medicaid recipient most likely need to go to their County Emergency Room if they come down with a cold, or need a Rx refill because private practices generally speaking do not accept a patient with straight Medicaid. To be transparent, I do see many reports at the ER event level and think to myself this probably could have been handled in a urgent care or office visit setting? If there was ever a new VAERS 2.0 I think the event levels could be better defined and not so ambiguous in this respect. I want vaccines pushed into the abyss and never return, but if VAERS was run honestly, it would knock the vaccine business on their ass and out of business. I digress, right now in this current scam, Dr. Hooker didn’t seem to do any data “cleaning” aka data modeling like the Denmark team did for their analysis. I doubt neither team did any up-coding and would have missed not serious, safe and effective cardiac arrests and deaths like these.:


Yeah so under coding is a big scam and I guess takes to much work and time to reconcile or I guess the VAERS data is ugly enough and we just roll with the data as is for these papers?
There was this other thing that was a little sad about this paper, but it was kind of mentioned towards the end, it’s the THROTTLING aka purposeful delay in publishing reports. Hooker and Jablonowski are getting pinched by the throttle scam more than they know. Sorry Brian for pointing this out, but it must be done…
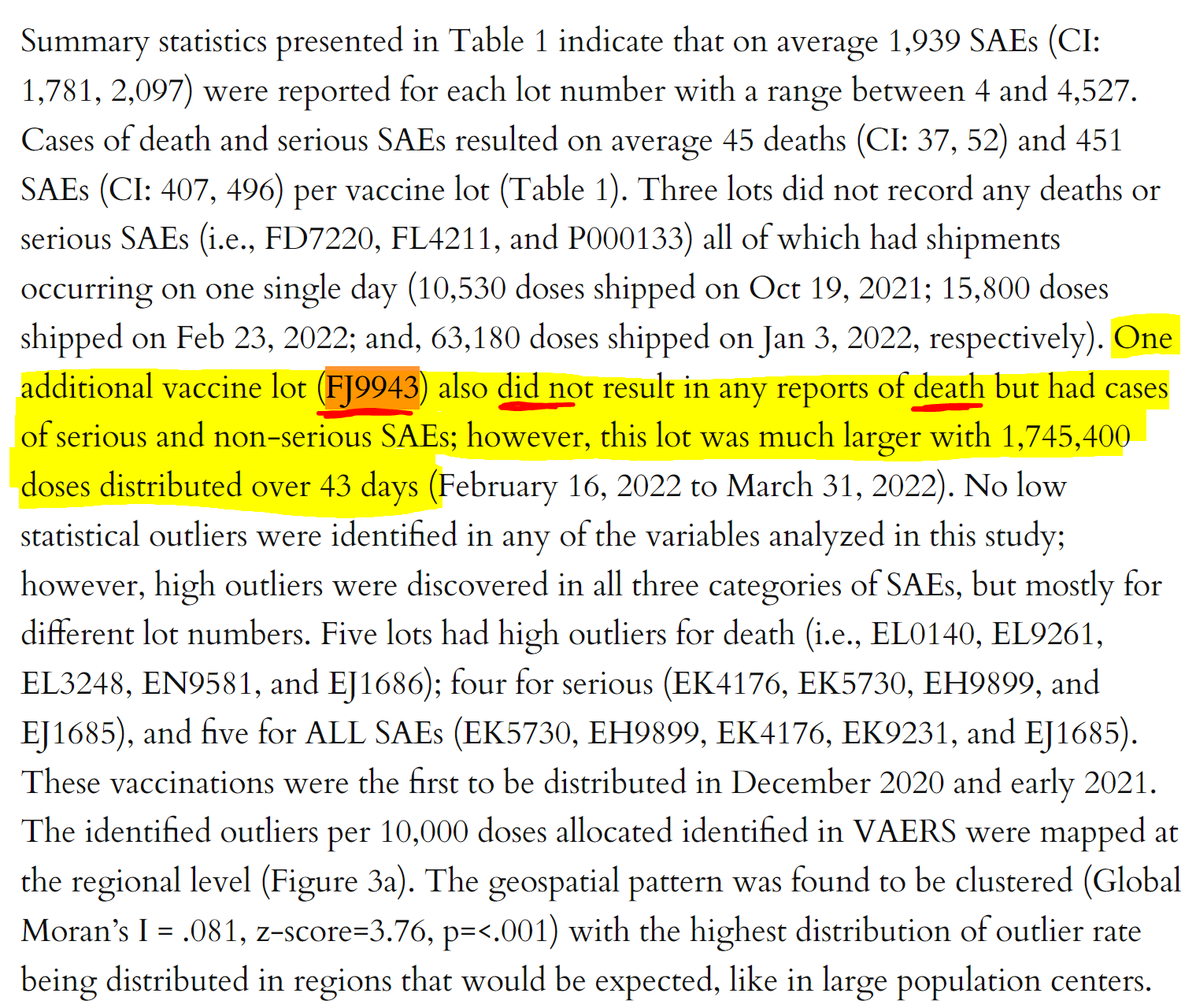
FJ9943 does have a death, but the throttle scam bit Dr. Hooker!
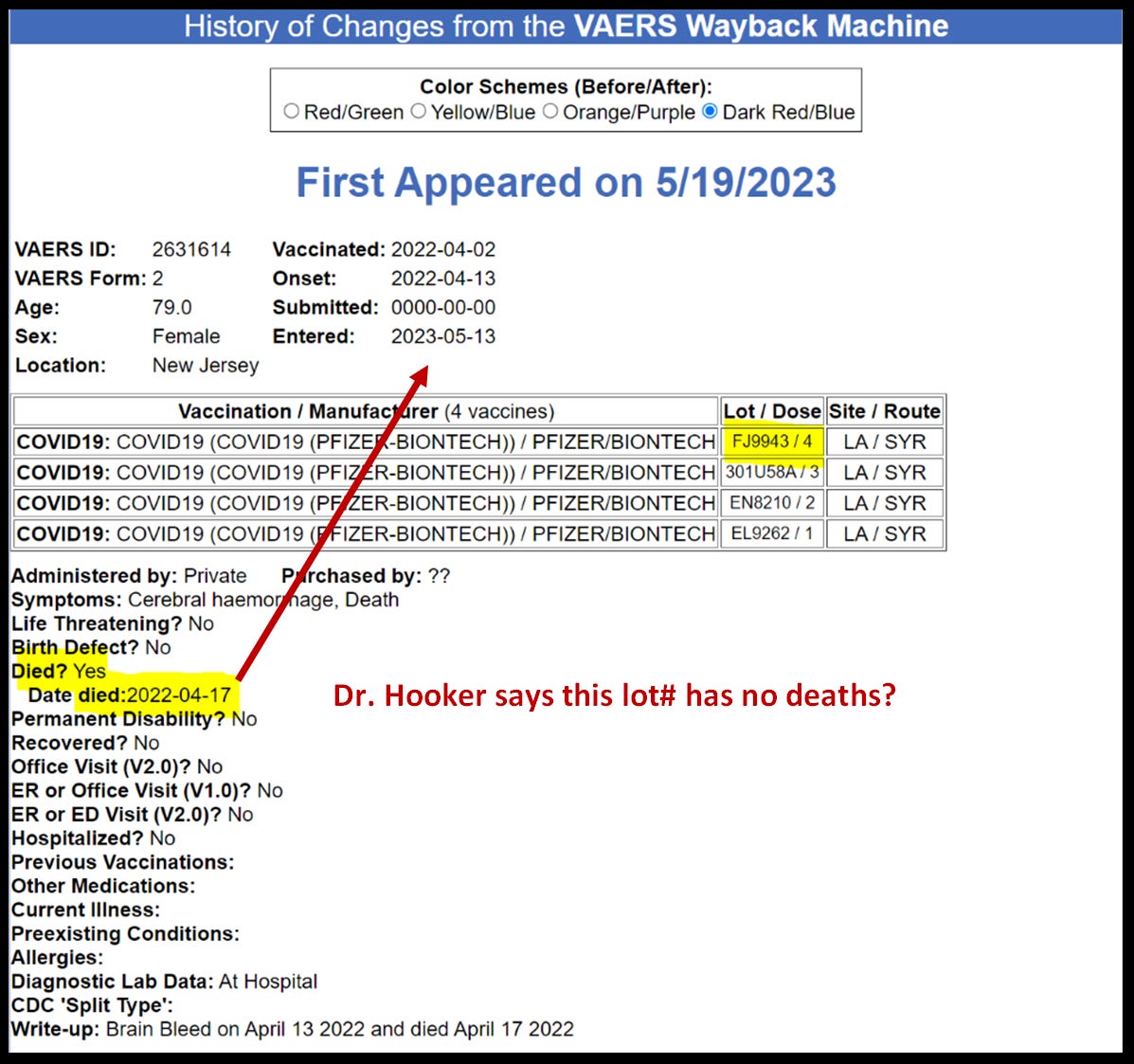
This lady died April 2022, but the report was not submitted to VAERS until a year later! Is this how they do things in Jersey hospitals? Regardless, this report has been sitting in VAERS for almost the last year and half. What version of VAERS is Hooker working from?
There is one more thing that in not precise in this paper for people that know the difference, it’s hard to distinguish when we are talking about vax dates, shipment dates, VAERS published dates, expiration dates, etc…
I understand this paper very well, in a matter of fact I appreciate it very much and it’s given me some ideas to re-visit a oldie but goodie dashboard I made July 16, 2023. Dr. Hooker just validated my ICAN Pfizer dashboard with this study!

I guess maybe it’s time to build another custom Pfizer ICAN dashboard and incorporate the scatter plots and blue, green, yellows groups that everybody likes so much.
I’m not sure why I applied the blue, green, yellow scatter plot technique for Moderna, and not for Pfizer at the time?

Yeah I don’t know, I guess I’m an enigma that way… This is a great study and Dr. Hooker even canoodled with the willful misconduct of under-coding and throttling or purposeful delay in submitting and/or publishing reports.
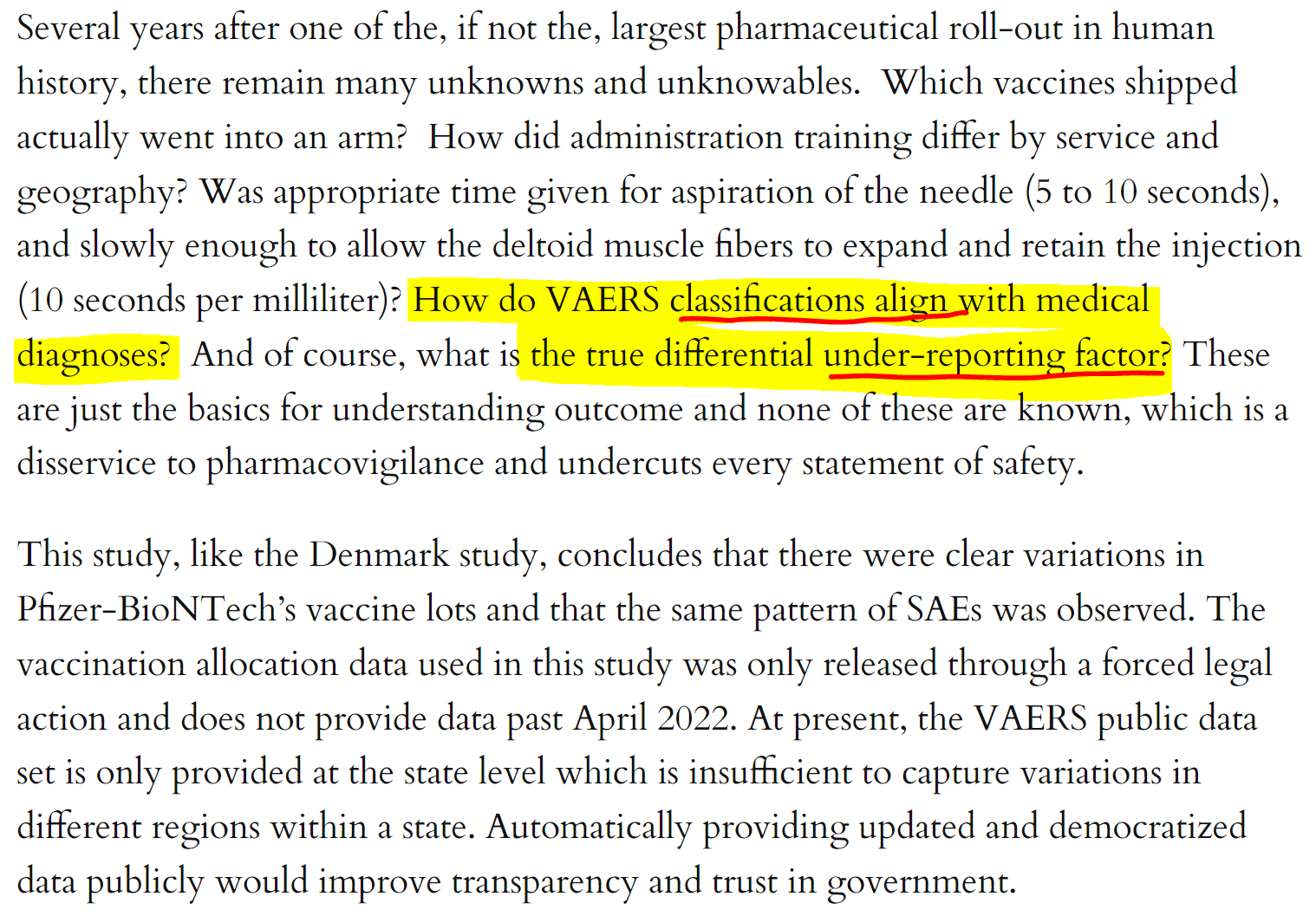
Don’t forget even Bobby knows VAERS ain’t publishing all legitimate reports received! I wonder if this is the under reporting Hooker is talking about?
I still love you Brian Hooker! I hope you still love me back? God Bless
Please support The Eagle!
Blessings to you WTE88 - thank you for the work you do by exposing TRUTH to medical tyranny ...
Hooker and Jablonowski said
"Six lots were excluded from the study as allocations likely continued past the study end date (see Supplemental Table 1). Also note that 28,170 doses, or 0.01 percent, had reported missing lot numbers." Have you looked at those 6 Lots Albert?