As of Saturday May 3, 2025 8:38am PST - CDC has not updated this months VAERS data? Highly unusual unless the “drop” dates fall on or near a major holiday.
Bottom line is there are some big changes underway and of course there is no alert or heads up from the CDC. This is like the opposite of radical transparency, so I’m still waiting for that ideology to be practiced. Let me just show you what Dr. Steven Rubin shared with me yesterday as I was eagerly waiting for the new files to drop.:
Email sent to me by Rubin yesterday at 2:28pm (PST):
I was expecting a VAERS release today, this being the first Friday of the month. Then three interesting things happened, one minor, one wonderful, and one annoying. First the minor: Nobody at VAERS updated their website today. They are supposed to modify the web page when they post new data, and it didn't happen. So by mid-afternoon, I tried downloading anyway. It's happened before: they post the data but forget to change the site to say it's been done. And yes, new data was waiting. Now the wonderful: VAERS has for a long time held additional versions of cases that were not part of the download. A case (such as VAERS ID 25006) would actually exist in multiple forms, 25006-1, 25006-2, and so forth. I always knew there were multiple versions because when I search VAERS on CDC Wonder, I see these extra digits at the end of the VAERS ID. But the downloads never had them. Suddenly today, these cases are part of the download (thank you, Bobby). There are over 70,000 new versions of existing cases. I believe these are follow-on versions with updated information. For example, case 25006 now has a follow-on case that looks mostly the same, but now states that the patient DID NOT recover. Now (sadly) the annoying. First of all, these download files are different, which requires some effort to reprogram. I managed to cobble-together a version of the software that ignores the follow-on cases, leaving me with the same-old VAERS, just updated by one month. Figuring out how to manage this extra data is going to require some consideration, and I'm open to suggestions. But worse (and truly puzzling to me) is that my website is not allowing me to install even this stripped-down release of the data. Something is wrong at MedAlerts.org and I can't figure it out. I don't think I've been hacked, but the website refuses to upload this new data, so I need professional help. In the meantime, sit tight. No new data at MedAlerts (and there's nothing at CDC Wonder, either). -Steve
5:53pm:
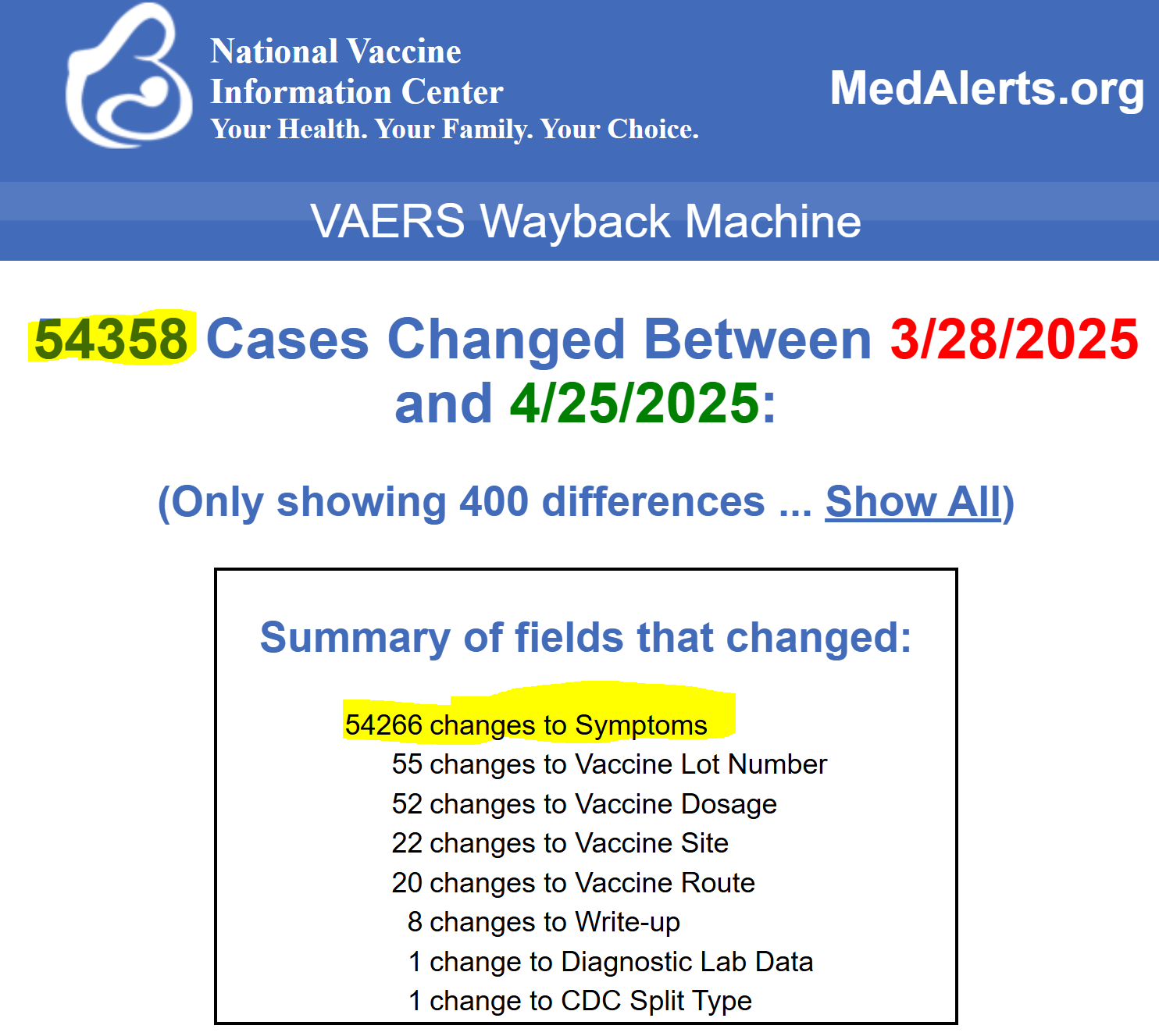
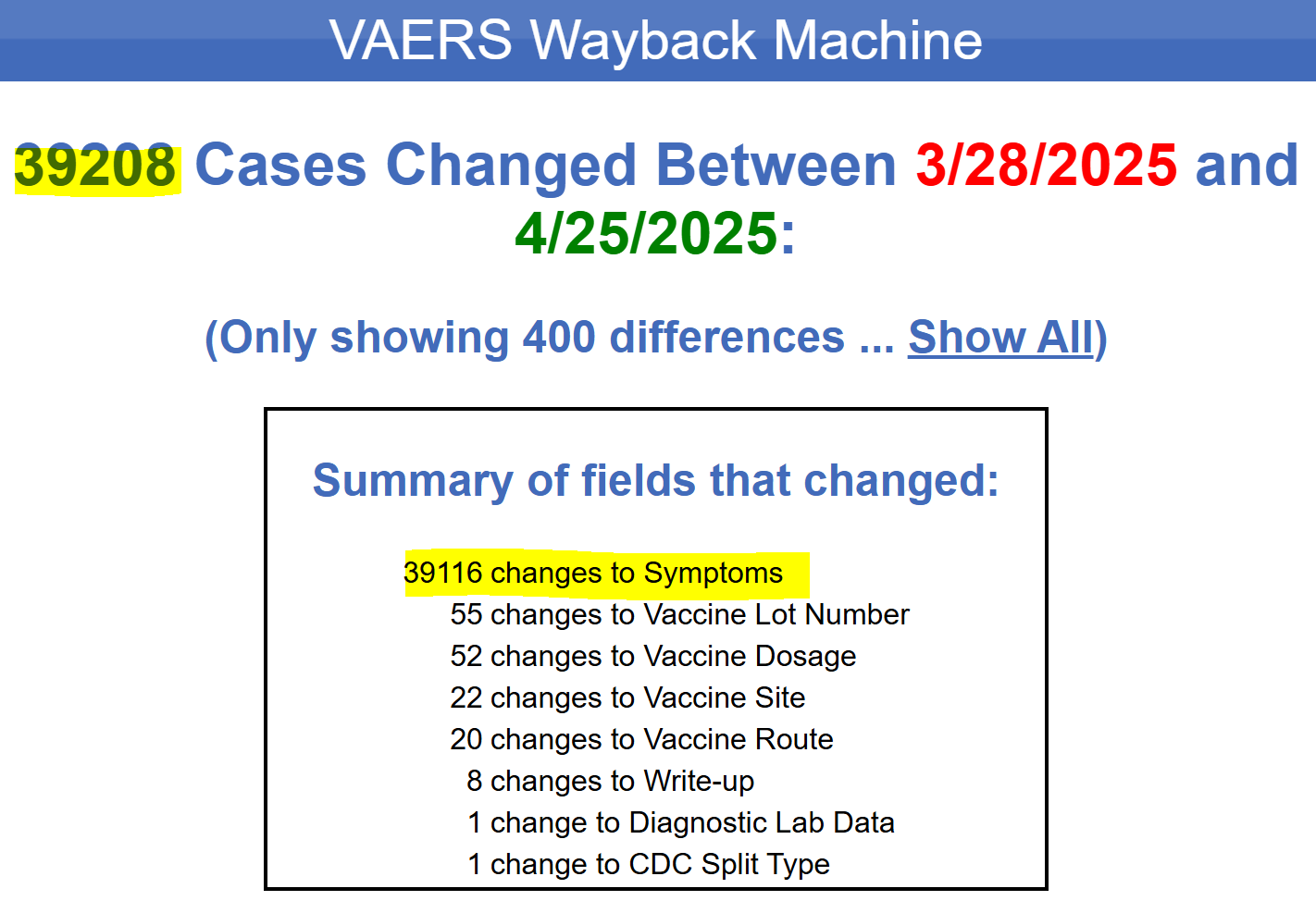
I found a bug in my new code and it now seems to be able to publish the new VAERS data. It's up at MedAlerts now. One downside of this data is that over 58,000 cases have had symptoms modified, often removed. This could also be a result of the new data release. I'll wait until CDC Wonder has this data to see if my interpretation is correct (they're still showing last month). But a far as the general state of things, the rest seems normal. Here is the automated report. -Steve
6:01pm:
My response:
Steven, Thanks for the updated. I've been waiting all day and checking every hour, but I didn't think to download anyways. I'm downloading whatever version they give me now to take a peak inside and follow your guidelines and I will proceed with caution. Please let me know if you discover anything else. Sincerely, Albert
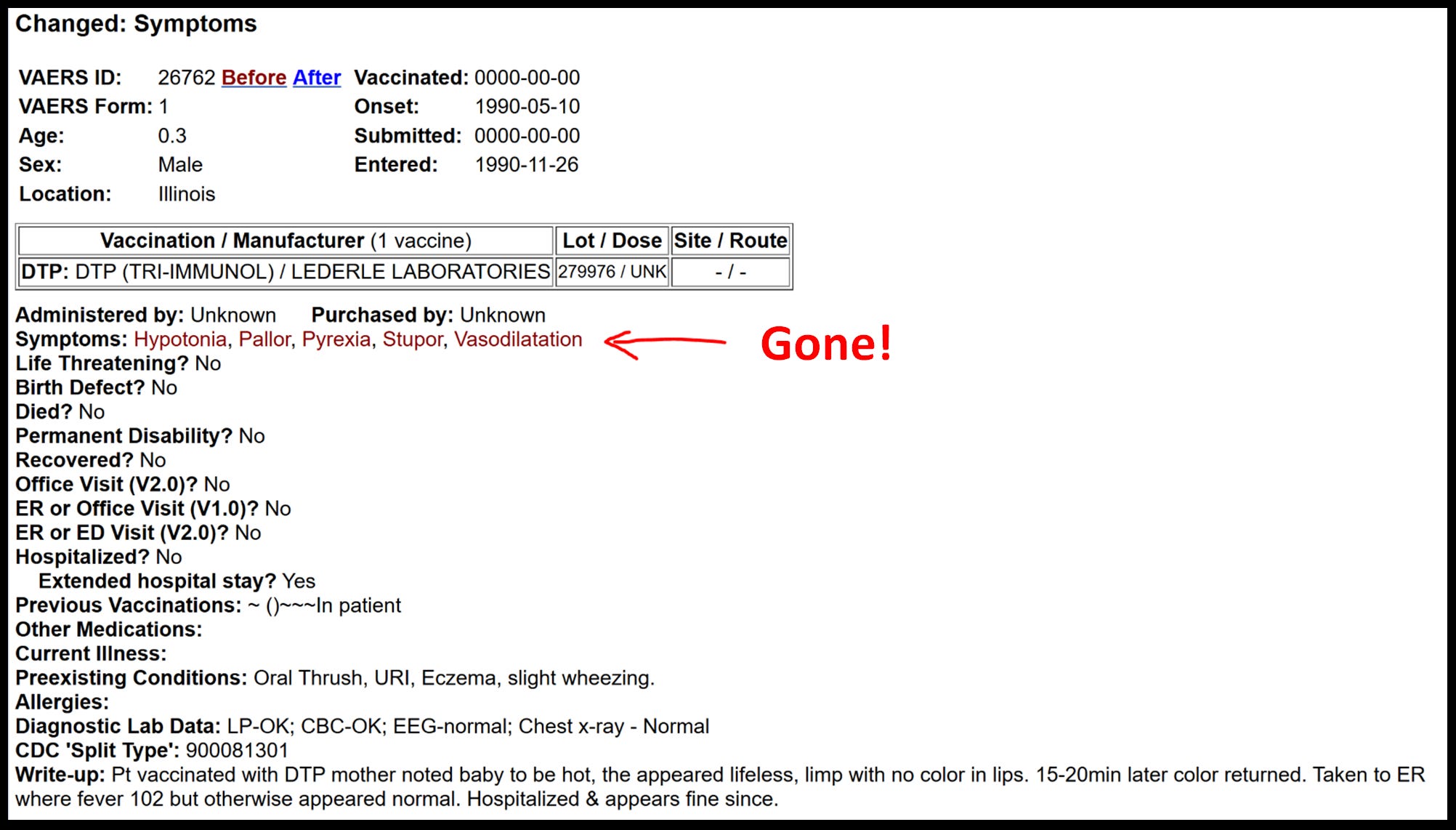
In practical application this is what it looks like CDC has done, of which it “looks” like they are scrubbing symptoms off old reports!
Updated 5/5/2025
Very few changes to symptoms are “good” meaning more are added or a better more descriptive symptom/diagnosis replaced a ambiguous symptom. Some reports look to have all symptoms wiped off entirely, leaving reports without medDRA codes at all.:
We don’t know what is going on until the dust settles and the CDC updates the WONDER SYSTEM with the official new VAERS data. They technically have not released the “new” downloadable data, but it is there even though time stamps don’t reflect the update. It’s possible that VAERS retracts this data on the backend and replaces with new files and nobody would be the wiser except to Dr. Steven Rubin and now myself. Thanks Steven. This is exactly how I caught that dead Alaskan baby that died within 6hrs bleeding from the eyes, ears, and nose from their covid shot around Thanksgiving 2021. That age would have been inappropriate by the way, and the report was never officially published! Johnny Su, Tom Shimabukuro, and Wolensky’s nasty finger prints are all over that one!
There’s a lot of forensic analysis that needs to be done, but here’s some quick malfeasance that always happens….
No new snappy pharmacovigilance system with AI and all the bells and whistles is going to address this malfeasance and willful misconduct, it’s just going to make it easier to hide the perps nasty finger prints!
BTW, I was quoted in CHD’s new article. I felt like I was sort of misquoted, but I DO NOT co-sign on Makary’s or Bobby’s “new” pharmacovigilance system bullshit. They need to arrest and incarcerate some nefarious actors within the CDC/FDA agencies, and run a honest VAERS system with accountability!
I got a lot more to say about this article and this subject. I care too much to care about if CHD will ever call me up for a quote again, but here is what I said for you to compare what was written…
Questions:
What are your thoughts regarding this reported change? Is it needed? Does it have the potential to be beneficial?
A "change" is not needed, a massive improvement of honesty within the VAERS administration is desperately needed. We have proof that VAERS does not publish all legitimate reports received. No amount of operation protocol improvements will help if the malfeasance and willful misconduct is allowed to exist at VAERS or some new Health Information Exchange. Technically a "Exchange" in the HMO or medical billing world is known as a "clearinghouse". These Exchanges receive medical billing data from CMS and other providers insurance claims which are then parsed and sent to their respective insurance carriers. A single hospital will send their hundreds or thousands of claims a day to their clearinghouse which will then parse and forward to hundreds of different insurance companies. Clearinghouses like OfficeAlly, Emdeon, McKesson, ChangeHealthCare, Athena are the largest in the USA. Even Medicaid's popular Vaccine For Children (VFC) program runs through clearinghouses/exchanges. However insurance claim exchange/clearinghouses are a moot point for vaccines if there are no sufficient ICD-10 codes for vaccine injuries. We can only capture a vaccine being administered in the insurance data, but we can not capture "myocarditis due to Covid-19 vaccines", "pulmonary embolism due to Covid-19, MMR, RSV", etc.
We can not capture "Death due to a vaccine like Covid-19"....
What are some of the limitations of VAERS? What are some of its advantages?
A arbitrary limitation of VAERS is only being allowed to publish initial reports, even though VAERS continues to capture follow-up data! Prior to January 2011 and the Harvard Pilgrim Study, VAERS did append follow-up data to initial reports and publish (update). See #4:
Another arbitrary limitation is the purposeful delay in publishing report and well beyond the initial 4-6 week adjudication window. Allowing typos and missing information errors to pass into publication is also a arbitrary limitation. Ages, vax dates, lot numbers, and death dates are clearly documented in the summary narratives of VAERS yet the applicable data field is not populated, and therefore populated with these missing data elements. Surely they address these oversights internally and ethically cleanse or correct missing data fields, but not for forward facing "public" VAERS. Any request for additional information during the initial adjudication phase is not being made public and when that information is obtained. Again it is arbitrary to only publish initial reports and without any additional information or ethical corrections have been done. Moot is arbitrary limitations if VAERS does not even publish all legitimate reports received. Even Robert F. Kennedy knows VAERS does not publish all legit reports. Bobby is the one who told my church here: https://x.com/welcometheeagle/status/1840060338529820688
VAERS Advantage: 1) It's public. 2) Offers downloadable raw data for further analysis 3) allows public to submit reports. 4) Allows public to submit follow-up data, however it's extremely difficult to navigate processes of sending additional data.
For a “lay” audience, what are Health Information Exchanges? What databases and what information do they potentially include?
As above, "Exchanges" are usually medical billing clearinghouses, but can include any entity sharing health information in a bi-directional manner. Custom electronic medical records (EMR) software can be tethered to billing software that are technically two different companies. The EMR and billing company now become an "exchange". VAERS, V-SAFE, FAERS, VSD are technically exchanges but they are not true bi-directional exchange of medical information.
How does active surveillance/real-time monitoring work in this instance?
Imagine I was Stanford University Hospital but some of my medical billing and coding people are in India. This is real time access and the slew of predefined queried analysis reports would be my monitoring. Real time surveillance would be like everybody in the USA having Master level access to EPIC. It would look no different if we are talking about radical transparency. The publics access level doesn't allow to see HIPPA sensitive data like date of birth, social security number, name, address, telephone number, copy of insurance card. It's not hard to do and we would not need to reinvent the wheel like Dr. Marty Makary might be suggesting.
How would you like to see this system work? What would you like to see done?
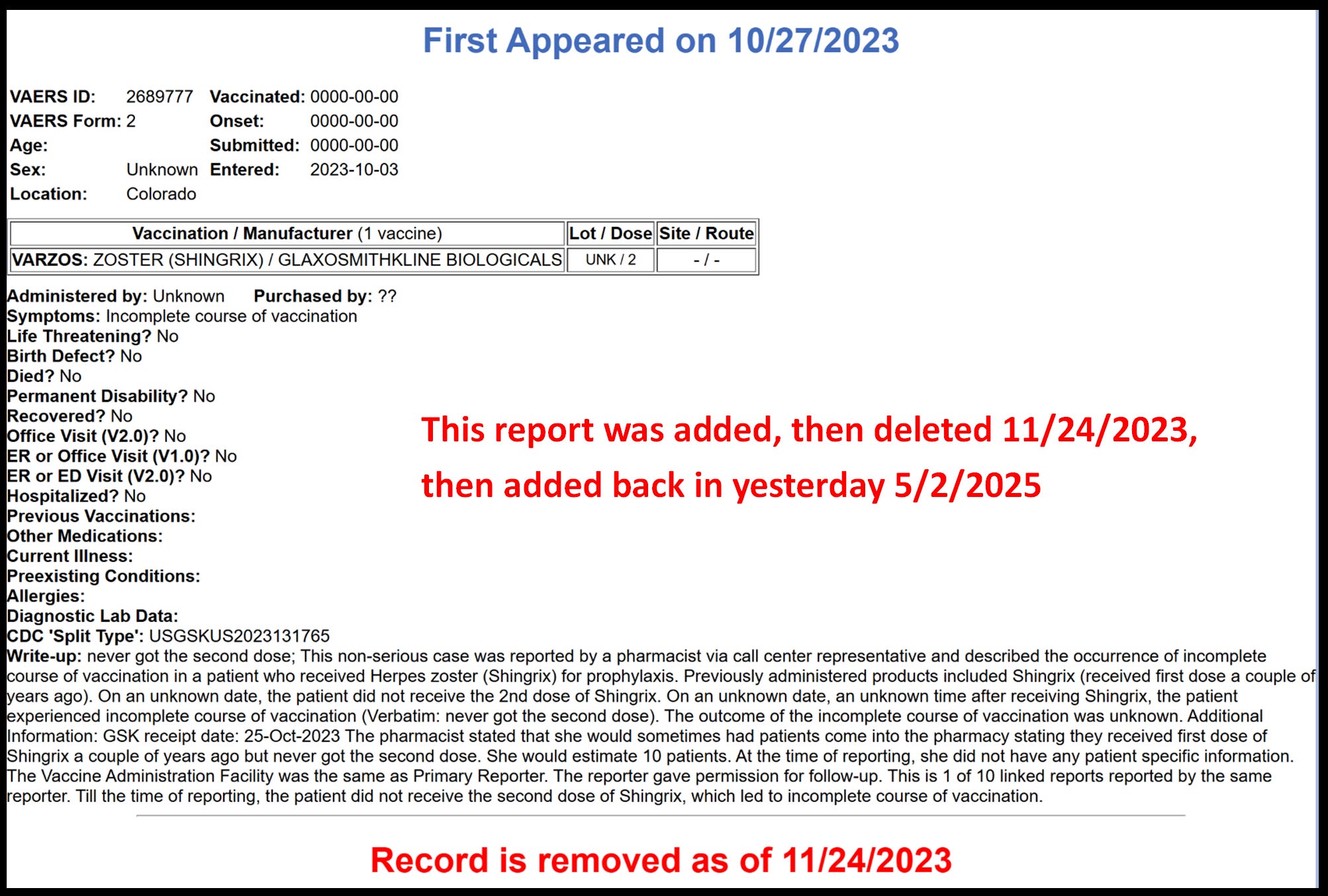
I'd like to see initial reports, and follow-up data. I'd like to see time stamps of corrected or appended data much like Barbara Loe Fisher and Dr. Steven Rubin's Medalerts.org captures. I would like to see less barriers for registrants submitting follow-up data and additional data. I would like to see a quick explanation for deleted reports. There are currently over 33,000 reports that have been published but later deleted and without explanation or any alert whatsoever. Many people we have identified in the react19.org community have had their report deleted without any explanation and no current "live" report exists! See here: https://www.react19.org/research-studies-surveys/react19-research-vaers-audit
I'd like to see interactive style dashboards with many data visualizations like vaersaware.com. Dashboards like ICAN's V-Safe except with all available filters.
I would like to see a correlation table between MedDRA (symptom) codes and ICD-10 codes. I would like to see low level details about submitter like who submitting any data element like Hospital, Skilled Nursing Facility, Urgent Care Clinic, County or state health department, manufacturer, military, patient or relative of patient registrant.
I would like to see race data. VAERS collects it but does not publish it.
I'd like to see a chain of custody and time stamps between Temporary ID# and Finalized ID#. Without visibility on temporary ID numbers it's impossible to know how many reports have been submitted, how many were not published due to duplicates, fake or frauds. without Temporary and Final ID correlation we do not have a sense of any "backlog" or inventory of reports "in-process"?
Are there any potential disadvantages or pitfalls to the proposed new system?
Not making the system public would be a huge mistake, at least VAERS is public as curated as it is. Any system needs accountability and enforcement. We would be in the realm of insanity doing the same closed system but expecting different results.
What might data from this new system show?
Raw data, analytics, and hopefully it will be more transparent about vaccine lot numbers and National Drug Codes (NDC) and race, etc. An honest pharmacovigilance system should show the truth. VAERS is showing signals even with partial truth of data, yet no governing body has ability to act on the unfavorable data?
Is there anything else you would like to add, not covered by the above?
More than anything, without sufficient ICD-10 to reflect injuries and death due to vaccines we will always be on this hamster wheel of speculation. If President Trump, Robert Kennedy Jr, Dr. Jay Battycharia, Dr. Makary, and the whole HHS want to act in the best interest of the people, they would do what needs to be done and create ICD-10 codes for vaccine injuries. Do we really live in a make believe world where vaccines have not caused a injury? Everything else is just a thinly veiled carnival trick or well choreographed Vegas show.
Above I was asked asked what how a active real time monitoring system work? I replied it’s a having master level access to the EPIC system…
Frankly I’m tired of people opining and getting sold on good ideas. I’m tired of PhD dump & pump professionals and computational biologists thinking they have all the answers.
Yo Bobby you are looking at entirely the wrong set-up of people for the answers. Don’t ask a shark to climb a tree. Let the sharks hunt in the ocean and let the monkeys climb the trees!
I had master access to EPIC and a some other cool systems. I had full access to 12 EMR’s all at once including Stanford Hospital. When CEO’s and CFO’s bullshit at Mari-Lago or on the golf course about what they want, they bring those request down the chain and it eventually hits people like me. Think of me like the quarterback or a coach.
Here was a cool Master Access to a Emdeon system for the 4th largest laboratory in the nation (Bio-Reference Laboratory) sending out 18K-22K insurance claims a day and receiving electronic reimbursements:
Here some E-Clinical Works:
AdvancedMD":
Lytec/McKesson:
Ge Centricity:
Here’s some analytics/visuals that could easily be customizable for pharmacovigilance system. When I think of pharmacovigilance I think of guys in the cockpit looking at stuff like this:
I knew VAERS was half baked but had no idea they were changing “ingredients” midstream, turning the oven off, then on, then off again during the baking process, and throwing screws into the blender while blending.














Any way YOU can please
campaign for the job to FIX this?
I knew VAERS was half baked but had no idea they were changing “ingredients” midstream, turning the oven off, then on, then off again during the baking process, and throwing screws into the blender while blending.
The Day Tapes
Richard Day
The science will be falsified.